








{kind=link}
 Ward Dean, MD
Ward Dean, MD
A 2014 study in the New England Journal of Medicine disparaged the lipid-lowering benefits of niacin and implied that it was actually toxic. The study in question was not a study of niacin, per se. It was actually a study comparing the addition of extended-release niacin plus laropiprant (an antihistamine which purportedly reduced niacin-induced flushing) to patients who were already taking simvastatin 40 mg per day, or simvastatin plus ezetimibe 10 mg per day (ezetimibe is a drug that is designed to increase HDL).1
I was really surprised to note that it wasn’t just a single article warning against niacin. The same issue of the New England Journal coincidentally had a Letter to the Editor, questioning the “Safety Profile of Extended-Release Niacin in the AIM-HIGH Trial,”2 and an Editorial, “Niacin and HDL Cholesterol – Time to Face Facts”3 — i.e., a triple take-out piece!
The study involved 25,637 high-risk patients from 245 test sites in the UK, Scandinavia, and China. The “placebo” group received Simvastatin 40 mg or Simvastatin 40 mg plus Ezetimibe 10 mg, plus a 50 mg low-dose niacin-containing “placebo.” The “Niacin” group received 2,000 mg of extended-release niacin and 40 mg of Laropiprant, in addition to the Simvastatin or Simvastatin plus Ezetimibe, as was given to the placebo group. The participants in the study were followed for a median of nearly four years. The study was stopped prematurely after three years because of an apparent lack of benefit with extended-release niacin (plus laropiprant).
The authors concluded that the Niacin-Laropiprant combination “did not significantly reduce the risk of major vascular events, but did significantly increase the risk of serious adverse harm,” and alleged that, “the study identified significant hazards, some of which had not been reported previously with niacin.”
Lipid-Lowering Effects of Niacin
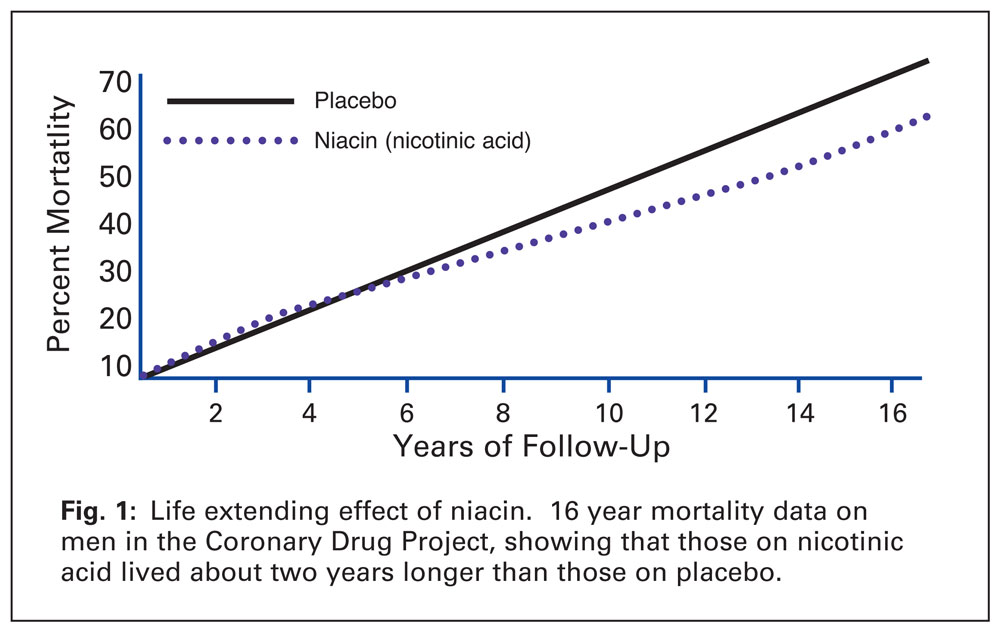
Let’s digress. The cholesterol-lowering effects of nicotinic acid were first reported in 1955.4The clinical benefits of immediate-release nicotinic acid were best demonstrated in the Coronary Drug Project (CDP), which compared immediate-release niacin with other cholesterol-lowering regimens on cardiovascular end points.5 In the CDP, immediate-release niacin reduced the total cholesterol level by 26 mg/dl (from a high baseline level of 253 mg/dl), and after six years, reduced the incidence of non-fatal MI (heart attacks) by 26% and cerebrovascular events (strokes) by 24%. Moreover, 9 years after trial termination, the group treated with niacin had 11% fewer deaths than the placebo group (Fig 1).5 Although lipid fractions were not measured in the CDP, subsequent studies with immediate-release niacin showed that it reduces LDL up to 25%, triglycerides up to 50% and Lp(a) up to 35%; and increases HDL up to 35%.6-8
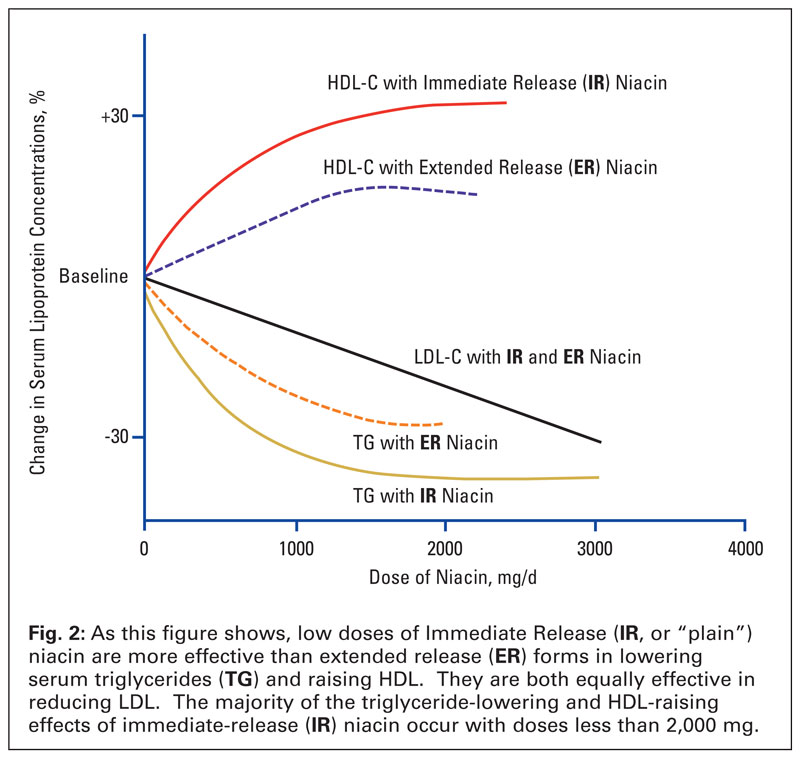
 The most commonly reported side effect of immediate-release niacin is the well-known flushing and itching of the skin (cutaneous vasodilation) that can be so uncomfortable that it may cause some people to discontinue taking it. Although the flushing can be overcome by taking niacin at the end of a meal, or by taking an aspirin 30 minutes prior to taking niacin, it is also self-limited, and tolerance to flushing develops with continued use. Nevertheless, pharmaceutical companies developed timed-release preparations to minimize or eliminate this effect. Unfortunately, timed-release niacin is less effective (and more toxic) than immediate release, cheap, over-the-counter niacin (Fig. 2).
The most commonly reported side effect of immediate-release niacin is the well-known flushing and itching of the skin (cutaneous vasodilation) that can be so uncomfortable that it may cause some people to discontinue taking it. Although the flushing can be overcome by taking niacin at the end of a meal, or by taking an aspirin 30 minutes prior to taking niacin, it is also self-limited, and tolerance to flushing develops with continued use. Nevertheless, pharmaceutical companies developed timed-release preparations to minimize or eliminate this effect. Unfortunately, timed-release niacin is less effective (and more toxic) than immediate release, cheap, over-the-counter niacin (Fig. 2).
Statin plus Niacin – Adverse Effects
Back to the New England Journal study. The “serious adverse harm” included “diabetes-related, gastrointestinal, musculoskeletal and skin-related disorders,” which the authors stated were previously known to be caused by niacin. Additionally, the authors stated that most of the serious musculoskeletal adverse events with niacin-laropiprant were due to myopathy (muscle weakness, pain and atrophy); and there was an unexpected finding of excess serious infection, and serious bleeding events. The authors further claimed that “niacin alone” was also associated with a significant increase in the risk of serious infection in a previous study as well (AIM-HIGH10).1
The AIM-HIGH study,10 however, was not a study of “niacin alone”—it was a study that also combined extended-release niacin with intensive statin therapy.
With regard to the excess bleeding, the authors conceded that it may not have been due to niacin—but may have been due to laropiprant – as several potential mechanisms for bleeding have been previously proposed for laropiprant,11,12 and niacin has not previously been reported to cause bleeding problems.
The authors of the New England Journal study curiously overlooked the fact that the FDA in 2012 required that labels on statin drugs be changed to include information concerning statin-induced glycemic effects, diabetes, and increases in hemoglobin A1C or fasting plasma glucose.13 This label change was based on several meta-analyses that demonstrated the relationship between statin use and diabetes. One meta-analysis examined the effect of statins on the risk of diabetes in 91,140 patients from 13 trials, which showed that statins were associated with a 9% increased risk of diabetes.14 Another meta-analysis of 32,752 patients, in five trials, found that higher potency statins were associated with a 12% increased risk of diabetes, compared to low potency statins.15Simvastatin, at a dose of 40 mg (as used in the New England Journal study), was considered to be a high potency statin.16
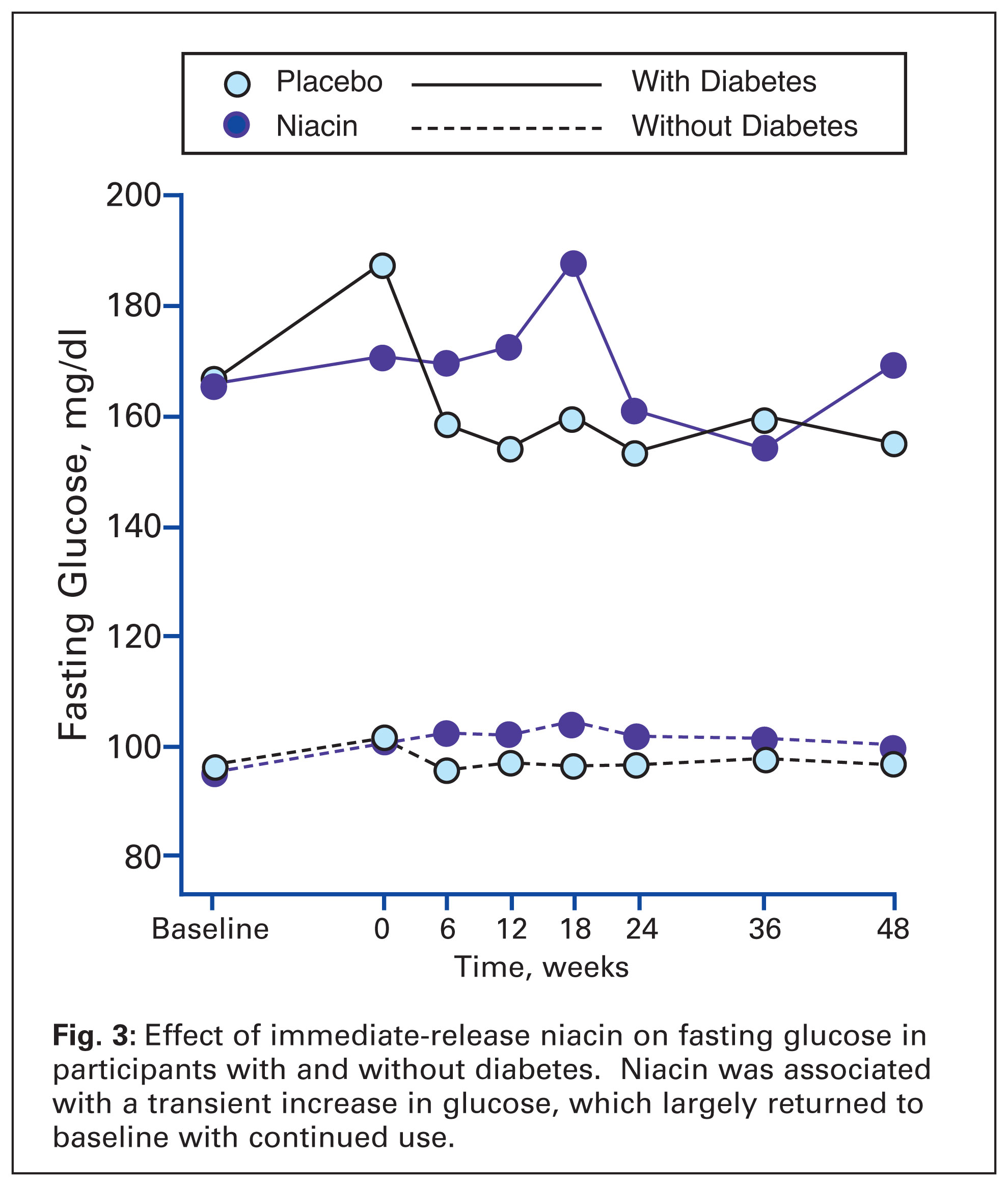
Although immediate-release niacin may cause reductions in glucose tolerance when treatment is initially begun, studies show that glucose generally returns to pre-treatment levels with continued use17,18 (Fig. 3). On the other hand, the package insert for extended-release niacin (as used in the New England Journal study) cautions that “NIASPAN can cause an increase in blood sugar levels.” It is thus likely that the combination of simvastatin and extended-release niacin in the New England Journal study caused the increased incidence of diabetic changes.
 Timed-release niacin also tends to be more hepatotoxic than immediate-release niacin, causing significant increases in liver enzymes, and multiple reports of hepatic failure.19,20One report, which illustrated the comparative safety of immediate-release niacin involved three patients who incurred hepatitis from timed-release niacin, who were later rechallenged with immediate-release niacin with no evidence of hepato-cellular injury due to the immediate release niacin.21
Timed-release niacin also tends to be more hepatotoxic than immediate-release niacin, causing significant increases in liver enzymes, and multiple reports of hepatic failure.19,20One report, which illustrated the comparative safety of immediate-release niacin involved three patients who incurred hepatitis from timed-release niacin, who were later rechallenged with immediate-release niacin with no evidence of hepato-cellular injury due to the immediate release niacin.21
Statins are known to cause myalgias, fatigue, and rhabdomyolysis. These effects may be worsened by combining statins with niacin. Most of the excess musculoskeletal adverse events in the New England Journal report were due to myopathy, and the absolute excess of myopathy associated with adding niacin-laropiprant to the statin-ezetimibe therapy was more than 10 times as great among participants in China as those in Europe.1 This should not have been surprising. The Zocor/Simvastatin package insert warns:
“Cases of myopathy/rhabdomyolysis have been observed with simvastatin coadministered with lipid-modifying doses (more than 1 g/day) of niacin-containing products. In particular, caution should be used when treating Chinese patients with simvastatin doses exceeding 20 mg/day coadministered with lipid-modifying doses of niacin-containing products.”
The New England Journal study concluded that “treatment with extended-release niacin-laropiprant did not significantly reduce the risk of major vascular events but did significantly increase the risk of serious adverse events.”1
The highly-publicized New England Journal article was thus not a true study of the clinical efficacy of over-the-counter immediate-release niacin. It was, instead, a testament that it’s probably not a good idea to combine extended-release niacin with a pharmaceutical hodge-podge of a high potency statins, ezetimibe, and latanoprost.
I’d like to see a head-to-head 3-arm study comparing the efficacy and side-effects of (1) immediate release niacin, (2) a statin, and (3) a statin plus niacin. Until such a study is conducted, I will continue to use (and recommend to my patients) immediate-release niacin—which I believe to be the safest, cheapest, most effective lipid-lowering substance available.
References
1. Landray, MJ, Haynes, R, Hopewell, J., et al. Effect of Extended-Release Niacin with Laropiprant in High-Risk Patients. NEJM, 2014, 371;3, 203-212.
2. Anderson, TJ, Boden, WE, Desvigne-Nickens, P, et al. Safety Profile of Extended-Release Niacin in the AIM HIGH Trial. NEJM, 2014, 371;3, 288-290.
3. Lloyd-Jones, DM. Niacin and HDL Cholesterol—Time to Face Facts. NEJM, 2014, 371;3, 271-273.
4. Altschul, R, Hoffer, A, Stephen, JD. Influence of nicotinic acid on serum cholesterol in man. Arch Biochem Biophys 1955; 54:558-9.
5. Canner, PL, Berge, KG, Wenger, NK, et al. Fifteen year mortality in Coronary Drug Project patients: Long term benefit with niacin. J Am Coll Cardiology 1986;8:1245-1255.
6. Miller, M. Niacin as a component of combination therapy for dyslipidemia. Mayo Clin Proceedings 2003;78:735-742.
7. Illingworth, DR, Stein, EA, Mitchel, YB, et al. Comparative effects of Lovastatin and Niacin in primary hypercholesterolemia. Arch Intern Med 1994; 154:1586-1595.
8. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High lood Cholesterol in Adults. Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults: Final report. Circulation 2002;106:3143-3421.
9. Knopp, RH. Drug treatment of lipid disorders. NEJM 1999;341:498-511.
10. The AIM-HIGH Investigators. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. NEJM 2011; 365:2255-67.
11. Lai, E, Schwartz, JI, Dallob, A, et al. Effects of extended release niacin/laropiprant, laropiprant, extended release niacin and placebo on platelet aggregation and bleeding time in healthy subjects. Platelets 2010; 21:191-8.
12. Dallob, A, Luo, WL, Luk, JM, et al. The effects of laropiprant, a selective prostaglandin D2 receptor antagonist, on the antiplatelet activity of clopidogrel or aspirin. Platelets2011;22:495-503.
13. Food and Drug Administration. FDA drug safety communication: important safety label changes to cholesterol-lowering statin drugs. 2012. www.fda.gov/drugs/drugsafety/ucm293101.htm
14. Sattar. M, Preiss, D, Murray, HM, et al. Statins and risk of diabetes; a collaborative meta-analysis of randomized statin trials. Lancet 2010;375:735-42.
15. Preiss, D, Seshasai, SR, Welsh, P, et al. Risk of diabetes with intensive-dose compared with moderate-dose statin therapy. JAMA 2011;305:2556-64.
16. Dormuth, CR, Filion, KB, Peterson, JM, et al. Higher potency statins and the risk of new diabetes: Multicenter, observational study of administrative databases. BMJ 2014; 348:g3244.
17. Elam, MB, Hunninghake, DB, Davis, KB, et al. Effect of niacin on lipid and lipoprotein levels and glycemic control in patients with diabetes and peripheral arterial disease. The ADMIT Study: A randomized trial. JAMA 2000;284:1263-1270.
18. Grundy, SM, Vega, GL, McGovern, ME, et al. Efficacy, safety, and tolerability of once-daily niacin for the treatment of dyslipidemia associated with type 2 diabetes. Arch Int Med2002; 162:1568-1576.
19. McKenney, JM, Proctor, JD, Harris, S. A comparison of the efficacy and toxic effects of sustained- vs immediate-release niacin in hypercholesterolemic patients. JAMA 1994;271:672-677.
20. Mullin, GE, Greenson, JK, and Mitchell, NC. Fulminant hepatic failure after ingestion of sustained-release nicotinic acid. Ann Intern Med 1989;76:239-241.
21. Henkin, Y, Johnson, KIC, and Segrest, JP. Rechallenge with crystalline niacin after drug-induced hepatitis from sustained-release niacin. JAMA 1990; 264; 241-243.
NIASPAN package insert, Revised: 04/2014