








A Natural Approach to Reducing Gastritis, Ulcers and Stomach Cancer
By Jim English and Ward Dean, MD
Helicobacter pylori (H. pylori) is a tiny bacterium that was completely unheard of twenty years ago. Today, H. pylori is known to afflict almost two-thirds of all humans, and is recognized as the most prevalent form of bacterial infection in the world. (1)
Residing in the stomach and duodenum of infected individuals, H. pylori is a spiral-shaped bacterium that has been strongly implicated in the development of gastrointestinal inflammation (gastritis) and gastric and duodenal ulcers. Now, new research strongly implicates H. pylori as the primary agent for development of gastric (stomach) cancer. Gum mastic is a natural substance from the sap of the Mediterranean evergreen tree, Pistacia lentiscus. Mastic gum has been shown to be effective in protecting the digestive system, healing peptic and duodenal ulcers, and eradicating H. pylori from the gut. Although it has not been clinically tested for this purpose, mastic gum offers a remarkable potential to effectively prevent stomach cancer.
Papa’s Got a Brand New Bug
 Gastric (stomach) and duodenal ulcers were once thought to be caused by spicy foods, stomach acid, and stress. This view was radically altered in 1982, when researchers in Australia discovered a new form of gram-negative bacteria in the stomach of patients with gastritis. (2) Dr. Robin Warren, a pathologist at the Royal Perth Hospital in Western Australia, first reported the unique spiral-shaped bacterium in biopsy specimens from patients with gastritis. Later, Warren and fellow Perth researcher Barry Marshall reported the presence of the new bacterium in virtually every biopsy specimen of 100 patients with duodenal ulcers.
Gastric (stomach) and duodenal ulcers were once thought to be caused by spicy foods, stomach acid, and stress. This view was radically altered in 1982, when researchers in Australia discovered a new form of gram-negative bacteria in the stomach of patients with gastritis. (2) Dr. Robin Warren, a pathologist at the Royal Perth Hospital in Western Australia, first reported the unique spiral-shaped bacterium in biopsy specimens from patients with gastritis. Later, Warren and fellow Perth researcher Barry Marshall reported the presence of the new bacterium in virtually every biopsy specimen of 100 patients with duodenal ulcers.
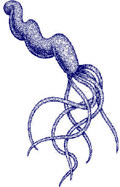
Predictably, traditional gastroenterologists initially rejected these new findings. In response to his critics, Warren swallowed a liquid culture of the bacteria, hoping to prove that H. pylori was the cause of peptic ulcers. Within weeks, he was diagnosed with a full-blown case of self-induced gastritis, proving his hypothesis was correct. In October, 1989, the new bacterium (previously called Campylobacter pylori) was officially recognized as a new genus and, due to its ability to occasionally take on the shape of a helix, given the new name Helicobacter (Fig. 1).
Mechanism of Action
Prior to the discovery of H. pylori, the stomach was thought to be a sterile environment. Indeed, a constant flood of digestive enzymes and concentrated hydrochloric acid makes the gut an extremely hostile environment for most pathogens. But research has revealed that H. pylori is uniquely adapted to take advantage of the hellish digestive brew. First, H. pylori uses its spiral shape and several whip-like tails (flagellae) to drill into the gastric mucosa –the mucus lining that protects the stomach and keeps it from being dissolved by its own gastric juices. Simultaneously, H. pylori produces a potent enzyme on its outer surface called urease. Urease protects H. pylori from being destroyed by gastric juices. Urease also disrupts the gastric mucus lining, making it easier for the bacteria to penetrate the layer and attach to the stomach and duodenum. Urease also protects H. pylori by converting urea (which is abundant in saliva and gastric juices) into a pair of strong bases – ammonia and bicarbonate. These, in turn, neutralize gastric acids – in effect, creating a protective antacid barrier around H. pylori.
H. pylori also defends itself from another immediate threat – the human immune system. The immune inflammatory response involves the production of vast numbers of neutrophils that are mobilized to destroy invading pathogens. Safely ensconced behind its mucus and antacid barriers, H. pylori is protected from attack by the immune system which cannot penetrate the mucus lining. Additionally, H. pylori produces another enzyme called catalase that further protects the bacteria from neutrophils. The result is that instead of repelling H. pylori, the immune inflammatory response causes severe damage to the stomach lining, thus contributing to gastritis and ulcer formation. (3)
Widespread Infection
While it is known that humans serve as the natural host of H. pylori, the exact mechanism of transmission is still unclear. Most researchers believe that infection occurs via oral-oral (kissing) or fecal-oral (food or water contamination) transmission. (4) In the United States only 20 percent of the population under 40 years of age is infected. But since infection continues to spread with time, the rate grows with each passing year until 50 percent of all US citizens over the age of 60 are infected. The infection problem is even greater outside of the US, with infection beginning early in childhood, leading to adult rates of infection approaching 90 percent in some parts of Asia and Africa. (5)
While many infected people may never show any symptoms, H. pylori is strongly associated with a number of gastrointestinal diseases, including chronic active, chronic persistent, and atrophic gastritis. Additionally, H. pylori infection is established to be a major cause of gastric ulcers (6) and up to 80% of all duodenal ulcers are blamed on H. pylori infection. (7) Since the immune system is helpless to control H. pylori, unless eradicated by other means, infection generally lasts a lifetime.
Stomach Cancer
Gastric cancer is the second most common cancer worldwide. In certain countries, such as Colombia and China, where H. pylori infects over half the population in early childhood, gastric cancer is the most prevalent form of cancer. (8) According to the National Institutes of Health (NIH) about 24,000 people in the United States are diagnosed with stomach cancer each year. (9) Of these, about 14,000 will die from the disease.
Data gathered from population studies had previously found an association between H. pylori infection and later development of a number of diseases, including 1) gastric mucosa-associated lymphoid tissue (MALT), 2) MALT lymphoma, 3) gastric cancer, 4) pancreatic cancer, 5) ischemic heart disease, 6) ischemic cerebrovascular disease, 7) atherosclerosis, 8) periodontal disease, and 9) skin diseases such as rosacea. (10)
Now, new research published in the September 13, 2001 issue of the New England Journal of Medicine confirms the hypothesis that H. pylori is the primary agent for the development of stomach cancer.
Japanese Study
H. pylori infection rates are much higher in Japan than in the US. Each year gastric cancer develops in 300,000 (0.5 percent) of the estimated 60 million infected with H. pylori. To study the link between H. pylori and stomach cancer, Japanese researchers enrolled 1,526 patients who suffered from ulcers, gastric hyperplasia, or non-ulcer dyspepsia (ulcer-like pain, but no ulcer). The study included 869 men and 657 women with an average age of 52 years. Patients underwent endoscopic biopsy at the time of enrollment, and at three years to assess H. pylori infection. They were monitored for an average of 7.8 years. Of the 1526 enrolled patients, a total of 1,246 (82%) were found to be infected with H. pylori. (11)
Over the course of the study 36 patients (2.9 percent) from the infected group developed stomach cancer. Gastric cancer did not develop in any of the uninfected patients. The researchers report that certain forms of gastric disturbance were associated with a higher risk of gastric cancer. Those patients most at risk were those with severe gastric atrophy (shrinkage and weakening of the stomach), gastritis (stomach inflammation), and abnormal intestinal tissue changes.
The researchers concluded that gastric cancer develops in persons infected with H. pylori, but not in uninfected persons. An accompanying editorial published in the September 13, 2001 New England Journal of Medicine stated that the findings “substantially bolsters evidence of the association” between H. pylori and gastric cancer, and suggest that “in the future, physicians may need to view H. pylori…as something akin to tobacco.” (12)
Eliminating H. pylori
Current medical protocols for eliminating H. pylori infection usually consists of a combination of one or two antibiotics (metronidazole, tetracycline, clarithromycin, amoxicillin), H2 blockers (cimetidine, ranitidine, famotidine, nizatidine), proton pump inhibitors (omeprazole, lansoprazole, rabeprazole) and bismuth subsalicylate, a stomach-lining protector. (10)
While these therapies can be effective, they are complex to administer, and are naturally expensive. Successful eradication of H. pylori is frequently compromised by patient noncompliance caused by unpleasant side effects (nausea, diarrhea and vomiting) and high costs of the drugs. Antibiotic resistance is also a growing problem that complicates treatment and increases risk of reinfection. (13)
Gum Mastic
For centuries, mastic gum has been used by traditional healers to treat stomach upset, ulcers, and heartburn. Modern research supports the use of mastic to restore and maintain proper gastrointestinal and digestive function. Research has shown that mastic is clinically effective in the treatment of benign gastric ulcers (14) and duodenal ulcers. In one double-blind clinical trial, researchers found that oral doses of one gram per day of mastic over a period of two weeks produced symptomatic relief in 80 percent of patients with duodenal ulcers. The study also found endoscopic evidence that mastic promoted the healing of gastric mucosal tissues. Ulcers were completely replaced with healthy epithelial cells. (15) Animal studies have also found that mastic possesses cytoprotective (cell protective) and antisecretory properties, and that it can reduce gastric mucosal damage caused by anti-ulcer drugs and aspirin. (16)
Mastic Eliminates H. pylori
Researchers writing in the December 24, 1998 issue of the New England Journal of Medicine reported that mastic is an effective antibacterial agent for the treatment of H. pylori. In the report the authors stated that, “Even low doses of mastic gum – one gram per day for two weeks – can cure peptic ulcers very rapidly… We have found that mastic is active against Helicobacter pylori, which could explain its therapeutic effect in patients with peptic ulcers.” (17)
The researchers conducted in vitro tests that revealed that mastic was effective in killing 99.9 percent of H. pylori when tested against seven different strains – NCTC 11637 (a standard reference strain) and six clinical isolates, including three resistant to metronidazole. Of note was the finding that mastic was equally effective against the drug resistant strains of H. pylori, even at very low concentrations. “These results suggest that mastic has definite antibacterial activity against H. pylori. This activity may at least partly explain the anti–peptic ulcer properties of mastic.'”
Conclusion
Mastic is an affordable and safe natural supplement that protects the digestive system, heals peptic and duodenal ulcers, and eradicates H. pylori from the gut. H. pylori is linked with gastrointestinal inflammation (gastritis) and gastric and duodenal ulcers. Research also implicates H. pylori as the primary agent for development of gastric stomach cancer. Gum mastic, because of its ability to eradicate H. pylori, may effectively prevent this common form of deadly cancer.
References
1. Cave, DR. How is Helicobacter pylori transmitted? Gastroenterology 1997 Dec;113(6 Suppl):S9-14.
2. Fukuda Y, Tomita T, Hori K, Tamura K, Shimoyama T, Nishigami T. The history of Helicobacter pylori. Rinsho Byori 2001 Feb;49(2):109-15.
3. http://www.glaxowellcome.ch/gw/fr/public/background_hp.
4. Cullen DJ, Collins BJ, Christiansen KJ, Epis J, Warren JR, Surveyor I, Cullen KJ. When is Helicobacter pylori infection acquired? Gut 1993 Dec;34(12):1681-2.
5. http://www.pasteur.ac.ir/biotechnology/infecdis.htm.
6. Xia HH, Yu Wong BC, Talley NJ, Lam SK. Helicobacter pylori infection – current treatment practice. Expert Opin Pharmacother 2001 Feb;2(2):253-66.
7. Peterson WL, Ciociola AA, Sykes DL, et al. Ranitidine bismuth citrate plus clarithromycin is effective for healing duodenal ulcers, eradicating H. pylori and reducing ulcer recurrence. Aliment Pharmacol Ther 1996;10:251-61.
8. http://www.cdc.gov/ulcer/md.htm
9. http://cancernet.nci.nih.gov/wyntk_pubs/stomach.htm.
10. Pakodi F, Abdel-Salam OM, Debreceni A, Mozsik G. Helicobacter pylori. One bacterium and a broad spectrum of human disease! An overview. J Physical Paris 2000 Mar-Apr;94(2):139-52.
11. Uemura N., Okamoto S., Yamamoto S., Matsumura N., Yamaguchi S., Yamakido M., Taniyama K., Sasaki N., Schlemper R. J. Helicobacter pylori Infection and the Development of Gastric Cancer. N Engl J Med 2001; 345:784-789, Sep 13, 2001.
12. Fox JG and Wang TC. Helicobacter pylori – Not a good bug after all. N Engl J Med 2001; 345:829-32.
13. M.R. Fattahi, M. Saberi-Firoozi, A.R. Saadat, S. Massarrat. Helicobacter pylori re-infection and recurrence rates of duodenal ulcer following treatment with three different anti-H. pylori regimens: A two-year follow-up study. Irn J Med Sci 1999; 24(3&4):82-86.
14. Huwez FU, Al-Habbal MJ. Mastic in treatment of benign gastric ulcers. Gastroenterol Jpn 1986;21:273-274.
15. Al-Habbal MJ, Al-Habbal Z, Huwez FU. A double-blind controlled clinical trial of mastic and placebo in the treatment of duodenal ulcer. J Clin Exp Pharm Physiol 1984;11:541-4.
16. Al-Said MS, Ageel AM, Parmar NS, Tariq M. Evaluation of mastic, a crude drug obtained from Pistacia lentiscus for gastric and duodenal anti-ulcer activity. J Ethnopharmacol 1986;15:271-278.
17. Huwez FU, Thirlwell D. Mastic Gum Kills Helicobacter pylori. N Engl J Med 1998; 339:1946, Dec 24, 1998.

-Lipoic Acid: Unique ‘Mitochondrial Antioxidant’ Fights Premature Aging")
{kind=link}