








By Jim English
One of the prospects facing otherwise healthy adults is the inexorable loss of memories and cognitive performance with advancing age. Aging baby boomers are becoming aware of age-related cognitive dysfunction, memory impairment and dementia. This growing problem is matched with an equally alarming increase in the number of adults being diagnosed with Alzheimer’s disease and Parkinson’s. A number of drugs and nutritional supplements have been proven to help slow the loss of cognitive functions in aging individuals. A growing body of research indicates that galantamine – a powerful new cognitive enhancing phytonutrient – is among the safest and most effective neuro-protective substances available today.
Dementia and the Aging Brain
All adults experience occasional lapses of memory, from misplacing car keys to temporarily forgetting a name. Dementia, by contrast, is a permanent and progressive disorder marked by profound memory impairment and loss of complex cognitive functions, including problem-solving, decision-making, spatial orientation, and communication.
Dementia can be caused by the ravages of advanced age, as well as neurological disorders (Alzheimer’s disease and Parkinson’s), vascular disorders (multi-infarct disease), inherited disorders (Huntington’s disease), and infections (viruses such as HIV). A common factor shared by all of these disorders is a reduction of blood and oxygen levels in the brain, which starves brain cells of fuel while damaging cell membranes and accelerating brain cell death.
Over time dementia can lead to depression, incontinence, disorientation, speech disturbances, tremors, muscle weakness, tinnitus, and loss of visual acuity and coordination. In time dementia victims are rendered incapable of functioning and require round-the-clock care. Currently dementia affects an estimated 8 percent of all adults over the age of 65, and up to an astounding 50 percent of people over the age of 80.
Alzheimer’s Disease
Alzheimer’s disease (AD), the most common form of dementia, usually surfaces after about 50 years of age. Symptoms of Alzheimer’s include the progressive erosion of memories, accompanied by the deterioration of mental performance, communication skills, abstract thinking and personality. Alzheimer’s afflicts approximately 40 percent of all individuals over the age of 85, accounting for some 4 million people in the US. Life expectancy following diagnosis of Alzheimer’s is only about 8 years.
Vascular Dementia
Vascular dementia (VaD), the second leading form of dementia, is caused when cerebrovascular disease impairs blood flow to the brain and starves cells of oxygen and vital nutrients. Common cerebrovascular events that precede vascular dementia include strokes, carotid stenosis and aneurysms. More than 700,000 Americans experience a major cerebrovascular event each year, usually in the form of a stroke. Additional subsets of vascular dementia caused by cerebrovascular disease include hereditary vascular dementia, multi-infarct dementia, post-stroke dementia, subcortical ischemic vascular disease and dementia, mild cognitive impairment, and degenerative dementias (including Alzheimer’s disease, frontotemporal dementia, and dementia with Lewy bodies). Vascular dementia is also often found present, to some degree, in cases of Alzheimer’s disease (mixed dementia).
The Aging Cholinergic System
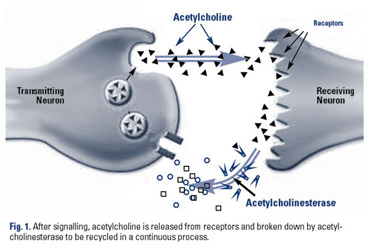
Central nervous system functions are controlled by the cholinergic system, a system of cells that produce and/or are stimulated by the neurotransmitter, acetylcholine. Two types of receptors – muscarinic and nicotinic – respond to acetylcholine to facilitate intracellular communication, memory processing and higher cognitive functions. The process begins when acetylcholine is released to travel across the synaptic cleft (Fig. 1) where it binds to a receptor on the other side of the synapse (post-synaptic terminal). Once the signal is triggered acetylcholine is rapidly broken down by an enzyme, acetylcholinesterase (AchE), and made available to be recycled.
Diminished cholinergic functioning, a biomarker of normal aging, is especially severe in cases involving dementia. In Alzheimer’s for example, amyloid plaque deposits in key components of the cholinergic system cause a drastic decline in acetylcholine levels. To make matters worse, already reduced acetylcholine levels continue to be degraded by AchE, further impairing memory and eroding cognitive ability. (1)
Reversing Cholinergic Decline
Conventional medical treatment for dementia involves drugs, called acetylcholinesterase inhibitors that suppress AChE to prevent it from degrading acetylcholine. This elevates acetylcholine levels and allows the neurotransmitter to persist in the synaptic cleft for a longer period of time. The two acetylcholinesterase inhibiting drugs currently approved for Alzheimer’s – Tacrine™ and Aricept™ – are only moderately effective and suffer drawbacks. Both are expensive, costing between $100 and $240 per month, and present serious side effects, including liver toxicity (Tacrine) to nausea and diarrhea (Aricept). (2)
Galantamine: Dual-Action Cholinesterase Inhibitor
Galantamine is a natural compound derived from the common snowdrop (Galanthus nivalis), a plant closely related to the daffodil. Galantamine first attracted attention when it was found to be an effective acetylcholinesterase inhibitor. Later it was discovered that galantamine amplifies the effects of acetylcholine by directly stimulating nicotinic receptors (nAChR). (3)
As stated earlier, nicotinic receptors are one of two types of receptors that are stimulated by acetylcholine. Nicotinic receptors are especially important for learning and short-term memory processes. Additionally, nicotinic receptors are damaged in Alzheimer’s disease, likely as a result of the build up of plaque on receptor sites. Obviously any compound that could stimulate these receptors would be of benefit in treating Alzheimer’s and other forms of dementia. Unfortunately drugs that act on nicotinic receptors tend to quickly desensitize the receptors, leading to tolerance and producing only short-term symptomatic improvement. (4)
As previously stated, in addition to acting as an acetylcholinesterase inhibitor, galantamine has also been shown to be a nicotinic agonist – an agent that mimics the effects of acetylcholine by directly stimulating nicotinic receptors. More importantly, galantamine was shown to be an allosteric modulator – a compound that interacts with receptors by binding to sites distinctly different from those used by acetylcholine or nicotine. Because allosteric modulators are not directly involved in the neurotransmission processes they affect, they do not induce compensatory processes that other compounds induce. Thus, problems such as receptor desensitization and down-regulation of expression are avoided. (5)
Unique Effects of Galantamine
Galantamine’s attributes result in a number of benefits not seen with other acetylcholinesterase inhibitors. First, acting as an allosteric modulator, galantamine stimulates nicotinic receptors and improves their functions without inducing tolerance and losing effectiveness. Second, galantamine amplifies the actions of acetylcholine to improve symptoms. Third, galantamine actually increases the release of acetylcholine, while modulating levels of other neurotransmitters involved in dementia, such as glutamate, serotonin and GABA. (6)
Human Studies
Numerous human studies support the use of galantamine to support cognitive function and memory. In one multicenter, double-blind, placebo controlled trial conducted in Europe and Canada, 653 patients with mild to moderate Alzheimer’s disease were treated with either galantamine or a placebo. After three weeks of therapy randomly assigned doses of galantamine were increased to maintenance levels of 24 or 32 mg per day. After six months, patients receiving galantamine showed significantly improved scores on an 11 item Alzheimer’s assessment scale compared to placebo. Patients on the higher doses also had significantly better scores on the dementia scale than the placebo group. Study authors concluded that galantamine slowed declines in functional ability and cognition, and was well tolerated by patients. (7)
In a second recent study, 285 patients diagnosed with Alzheimer’s disease and cerebral vascular disease participated in a multicenter double-blind study in England. Patients received either 24 mg per day of galantamine or a placebo for six months. Following the double-blinded phase, 238 patients continued the study, receiving 24 mg per day for the next six months. At the end of the one-year trial patients treated with galantamine showed clinically significant improvements in cognitive functions after six months and maintained their cognitive functions for the entire 12-month study. In contrast, cognitive functions deteriorated among those in the placebo group. When the placebo-treated patients began to take galantamine during the open-label phase of the trial they did show improvements in cognitive function, but they never attained the same cognitive level as patients who had been treated with galantamine for the entire 12 months. (8)
Conclusion
Aging adults face the loss of cognitive powers and impaired mental functions. Research supports the role of galantamine in slowing brain aging and preserving cognitive functions. Research also indicates that maximum protective benefits are observed when treatment begins before signs of irreversible declines in mental abilities.
References
1. Watkins PB, Zimmerman HJ, Knapp MJ. Hepatotoxic effects of tacrine administration in patients with Alzheimer’s disease. JAMA 1994 Apr 6; 271:992-8.
2. Watkins PB, Zimmerman HJ, Knapp MJ. Hepatotoxic effects of tacrine administration in patients with Alzheimer’s disease. JAMA 1994 Apr 6; 271:992-8
3. Doggrell SA, Evans S. Treatment of dementia with neurotransmission modulation. Expert Opin Investig Drugs. 2003 Oct;12(10):1633-54.
4. Maelicke A. Allosteric modulation of nicotinic receptors as a treatment strategy for Alzheimer’s disease. Dement Geriatr Cogn Disord 2000 Sep;11 Suppl 1:11-8.
5. Maelicke A, Samochocki M, Jostock R, Fehrenbacher A, Ludwig J, Albuquerque EX, Zerlin M. Allosteric sensitization of nicotinic receptors by galantamine, a new treatment strategy for Alzheimer’s disease. Biol Psychiatry 2001;49:279-88.
6. Samochocki M, Hoffle A, Fehrenbacher A, et al. Galantamine is an allosterically potentiating ligand of neuronal nicotinic but not of muscarinic acetylcholine receptors. J Pharmacol Exp Ther. 2003 Jun;305(3):1024-36. Epub 2003 Mar 20.
7. Efficacy and safety of galantamine in patients with mild to moderate Alzheimer’s disease: multicentre randomised controlled trial. Galantamine International-1 Study Group. BMJ 2000 Dec 9;321(7274):1445-9.
8. Bullock R, Erkinjuntti T, Lilienfeld S, GAL-INT-6 Study Group G. Management of Patients with Alzheimer’s Disease plus Cerebrovascular Disease: 12-Month Treatment with Galantamine. Dement Geriatr Cogn Disord. 2004 [Epub ahead of print]. Epub 2003 Oct 13.

-Lipoic Acid: Unique ‘Mitochondrial Antioxidant’ Fights Premature Aging")
{kind=link}
[…] is a natural nootropic compound which helps to boost overall cognitive functionality, enhance brain sharpness and promote mental recreation. Galantamine is an alkaloid prepared from […]
[…] 1. English J. Galantamine: preserving memory and cognitive function. Nutrition Review Archive 2013 https://nutritionreview.org/2013/04/galantamine-preserving-memory-cognitive-function/ […]